

TRANSFACET JOINT FIXATION
1. 1945: Facet screws - First screws to fixate the spine.
2. Published fusion and clinical excellence of 90%+
A LESS Exposure Advanced Spine Technology (LEAST™)
FacetFuse is a proven transfacet pedicle screw fixation technology for percutaneous spine fusion in outpatient settings. Wholly owned by NANISX LLC (a KIC Ventures portfolio company), FacetFuse is designed for LESS™ invasive lumbar stabilization, providing secure fixation while avoiding traditional open fusion complexity.
Unlike traditional pedicle screws, FacetFuse uses a direct transfacet technique to achieve compression and immediate stability. A biomechanical study shows two FacetFuse screws match the stability of four pedicle screws and offer superior immediate stability to unilateral pedicle screws. FacetFuse is effective as a standalone facet fusion or support for interbody cages.
Guided by LESS™ REP principles - Restore Function, Early Intervention, and Preserve Anatomy, FacetFuse enables safer, faster, and more efficient interventional spine surgery fusions. With clinical success, growing adoption, and expanding reimbursement coverage, FacetFuse is redefining outpatient lumbar fusion in ambulatory surgery centers (ASCs) and office-based labs (OBLs).
PROVEN
%20proven%20%20bone%20fusion.png)
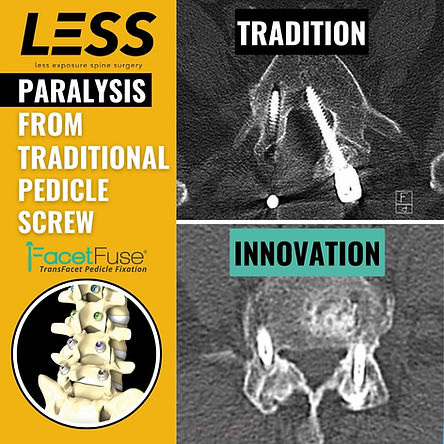
Learn why FacetFuse compresses obliquely across the facet joints vs spanning the joint with 2 traditional pedicle screws and a rod which leads to stress shielding which is bad for bone healing !
AO Principles of Fusion
The Arbeitsgemeinschaft für Osteosynthesefragen (AO) principles for fusion are a set of guidelines for improving fracture treatment results using internal fixation.
The AO principles of joint fusion include:
-
Accurately and closely fitting the fusion surfaces
-
Positioning the joint optimally
-
Maintaining bone apposition in an undisturbed fashion
-
Removing all cartilage, fibrous tissue, and other material that may prevent bone surfaces from contacting
The AO group was formed in 1958 by Maurice E. Müller, who was inspired by the work of Robert Danis on internal fixation and primary bone healing.
Wolff's Law of Fusion
Wolff's law states that bones adapt to the forces applied to them, becoming stronger or weaker over time. This law was developed by German surgeon Julius Wolff in the 19th century.
How Wolff's law works
-
Bones are constantly remodeling, replacing old or damaged bone with new bone
-
When bones are under pressure, osteoblasts produce more bone to strengthen it
-
Bones that are not under stress become thinner and weaker
HISTORICAL JOURNEY TO FACETFUSE
-
Dr. King introduced the first facet screws in 1945 for spinal fusion and in 1948, he published the use of short screws placed transversely across the facets.
-
Boucher (1959) pioneered screws placed across the facets through the pedicle into the vertebral body
-
Magerl (1984) introduced screws placed translaminar across the facets, advancing stability and fusion techniques.
-
FacetFuse transfacet screw, FDA-cleared in 2008 and introduced by Dr. Kingsley Chin, was a breakthrough in spinal fusion. It featured the world’s first multiaxial washer integrated onto the screw head, addressing the limitations of earlier techniques by providing enhanced flexibility and stability during fusion procedures.
KEY BENEFITS


-
LESS invasive with a less than 1-inch incision and minimal blood loss.
-
Nearly 13,000 successful implantations backed by published data.
-
Superior immediate stability over unilateral pedicle screws and rod constructs.
-
Comparable stability to bilateral screws and rods.
-
Over 90% fusion rates with no adjacent segment breakdown.
-
Easy and safer medial to lateral trajectory away from the spinal canal.
-
Designed for percutaneous outpatient spine fusion.
-
Broaden applications:
-
L5-S1 fusions
-
Post-laminectomy
-
Adjacent to prior lumbar fusion
-
Indications For Use (IFU)
FDA-Cleared since 2008
The FacetFuse® Screw Fixation System is intended to stabilize the spine as an aid to fusion by transfacet fixation. The subject device is indicated for posterior surgical treatment of any or all of the following at the L1 to S1 (inclusive) spinal levels including:
-
Trauma, including spinal fractures and/ or dislocations;
-
Spondylolisthesis;
-
Spondylolysis;
-
Pseudoarthrosis or failed previous fusions which are symptomatic or which may cause secondary instability or deformity;
-
Degenerative diseases which include
(a) degenerative disc disease (DDD) and/or (b) degenerative disease of the facets with pain and/or instability on plain flexion and extension lateral radiographs where there is movement of the vertebral bodies relative to each other of more than 4mm.
FACETFUSE FEATURES



.png)

COMPETITION

PEDICLE SCREWS VS FACETFUSE


FACETFUSE OBLIQUE TECHNIQUE





FACET SCREW CASE ILLUSTRATIONS
1-Level
Facet Fusion

2-Level
Facet Fusion

Adjacent Segment Disease








By: Dr. Doug Beall



PARS REPAIR

The incidence of spondylolysis has been shown to be 6% in the general adult population. The incidence is significantly higher in the athletic population, with studies showing as many as 52% of athletes with low back pain suffering spondylolysis and 60% with low back pain suffering a pars interarticularis defect of any grade. Other studies show that spondylolysis and spondylolisthesis constitute 47% of low back pain in adolescent athletes.
The Incidence of Pars Interarticularis Defects in Athletes.
Tawfik S, Phan K, Mobbs RJ, Rao PJ.Global Spine J. 2020 Feb;10(1):89-101. doi: 10.1177/2192568218823695. Epub 2019 Feb 24.

PARS REPAIR TECHNIQUE





CODING AND BILLING
